Gingival And Periodontal Health in
Systemic Lupus Erythematosus
The article I choose to summarize compares the periodontal health of patients with Systemic Lupus Erythematosus(SLE) and patients without. The study matched up the clients by age and sex with clinical and laboratory signs of SLE, and with diagnosed SLE. Patients with SLE were receiving inimunomodulatory therapies such as; corticosteroids, non-steroidal anti-inflammatory drugs, and showed no lesions around the gingiva. These were considered a controlled group. Assessments of gingival and periodontal health were determined by plaque indices and periodontal probing depths with a calibrated periodontal probe. The results showed the patients with SLE had lower probing depths compared to healthy patients. Comparison of the probing depths in SLE patients taking immunomodulatory drugs compared with those not using medications or using other drugs showed there was no influence on the drugs.
In conclusion patients with SLE have similar gingival and plaque indices as healthy patients but have lower probing depths. Its unclear why but is thought that it may be that periodontal micro flora of patients with SLE have lower pathogenicity or due to the effects of the long term administration of non-steroidal anti-inflammatory or immunosuppressive drugs.
How this will help me with DH care, and personal reflection
I think it will be important as a dental hygienist to be able to explain to my patient who might have Lupus reasons behind why there probing depths are low, but suffer from other issues in there mouth, such as painful ulcers, xerostomia, hypo salivation. I chose this condition because my son's great grendma has lupus. She is in her late seventy's, very out going and loves to be outside, I was definitly intrigued by this considering people who suffer from Lupus are supposed to stay out of the sun. Lupus very rarly get her down but when it does she is really out for the whole day. I think this disease can be debilitating, and I
would want to do anything I could to assure my patient that we can maintain there mouths, and do my best to keep them in optimal health.
Additional Information
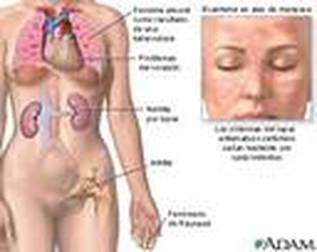
Systemic Lupus Ertheratousus is an autoimmune disease that affects tissue and organs. There are numerous different lesions associated with SLE including, root canal calcification, delayed primary and permanent tooth eruption, and twisted root formation. Oral mucosal lesions include discoid lesions, erythematous ulcerations, angular cheilitis, mucositis and glossitis. Lupus is an acute and chronic inflammatory autoimmune disease where the immune system fights the body that is supposed to protect. It affects mostly women in the childbearing years with the average age being 31. SLE is the most common form usually found on the gingiva, buccal mucosa, tongue and palate. Some complications that arise from Lupus are; Pulmanary Hypertension, inflammation of the blood vessels in the brain, and hardening of the arteries.
APA
Mutlu, S., Richards, A., Maddison, P., & Scully,
C. (1993). Gingival and periodontal health in systemic lupus erythematosus.
Community Dentistry & Oral Epidemiology, 21(3), 158-161.
doi:10.1111/1600-0528.ep12045415
Michele , D. , & Walsh, M. (2010). Dental Hygiene Theory and
Practice. (3rd ed.). canada: Linda Duncan
The article I choose to summarize compares the periodontal health of patients with Systemic Lupus Erythematosus(SLE) and patients without. The study matched up the clients by age and sex with clinical and laboratory signs of SLE, and with diagnosed SLE. Patients with SLE were receiving inimunomodulatory therapies such as; corticosteroids, non-steroidal anti-inflammatory drugs, and showed no lesions around the gingiva. These were considered a controlled group. Assessments of gingival and periodontal health were determined by plaque indices and periodontal probing depths with a calibrated periodontal probe. The results showed the patients with SLE had lower probing depths compared to healthy patients. Comparison of the probing depths in SLE patients taking immunomodulatory drugs compared with those not using medications or using other drugs showed there was no influence on the drugs.
In conclusion patients with SLE have similar gingival and plaque indices as healthy patients but have lower probing depths. Its unclear why but is thought that it may be that periodontal micro flora of patients with SLE have lower pathogenicity or due to the effects of the long term administration of non-steroidal anti-inflammatory or immunosuppressive drugs.
How this will help me with DH care, and personal reflection
I think it will be important as a dental hygienist to be able to explain to my patient who might have Lupus reasons behind why there probing depths are low, but suffer from other issues in there mouth, such as painful ulcers, xerostomia, hypo salivation. I chose this condition because my son's great grendma has lupus. She is in her late seventy's, very out going and loves to be outside, I was definitly intrigued by this considering people who suffer from Lupus are supposed to stay out of the sun. Lupus very rarly get her down but when it does she is really out for the whole day. I think this disease can be debilitating, and I
would want to do anything I could to assure my patient that we can maintain there mouths, and do my best to keep them in optimal health.
Additional Information
Systemic Lupus Ertheratousus is an autoimmune disease that affects tissue and organs. There are numerous different lesions associated with SLE including, root canal calcification, delayed primary and permanent tooth eruption, and twisted root formation. Oral mucosal lesions include discoid lesions, erythematous ulcerations, angular cheilitis, mucositis and glossitis. Lupus is an acute and chronic inflammatory autoimmune disease where the immune system fights the body that is supposed to protect. It affects mostly women in the childbearing years with the average age being 31. SLE is the most common form usually found on the gingiva, buccal mucosa, tongue and palate. Some complications that arise from Lupus are; Pulmanary Hypertension, inflammation of the blood vessels in the brain, and hardening of the arteries.
APA
Mutlu, S., Richards, A., Maddison, P., & Scully,
C. (1993). Gingival and periodontal health in systemic lupus erythematosus.
Community Dentistry & Oral Epidemiology, 21(3), 158-161.
doi:10.1111/1600-0528.ep12045415
Michele , D. , & Walsh, M. (2010). Dental Hygiene Theory and
Practice. (3rd ed.). canada: Linda Duncan
Google Image

Google Image
